The Pharmacokinetics and Mechanisms of Growth Hormone Dosing (why EOD GH is better than ED GH)

From your time here on X within the enhanced space, you may heard heard many opt for the use of exogenous growth hormone (GH or HGH), seeing them take the compound every day (or night) as part of a general or injury recovery protocol

However, this every day dosing carries with it the naivety of thinking "I must take this compound every day/night to get the best out of it." They may possibly think that the compound needs daily dosing by word-of-mouth/ear/anecdote that many others prior to them have used it, or from observing a professional bodybuilder talk about their use of GH
This naive assumption is incorrect because said people do not understand the pharmacokinetics and mechanisms behind GH dosing, which I will explain upon, as well as other fallacies.
There is a analogy for the layman at the very end
-----
GH Pharmacokinetics: The Three-Layer Temporal Model
GH is typically injected subcutaneously, with a serum/plasma half-life of ~3-4 hours (having a Tmax [time to reach maximum concentration] of ~2-4 hours), reaching effective clearance (where ~3% of GH remains in serum) by ~15-20 hours. But the biological active window is far longer due to the pharmacokinetic cascade:
Free, uncomplexed IGF-1 has a half-life of only ~10 minutes, and free IGFBP-3 of ~30–90 minutes. The extended circulating half-life is entirely a property of the ternary complex. This means a single dose of exogenous GH creates a 15–24+ hour window of elevated IGF-1 bioactivity: essentially leaving no meaningful "trough" with ED dosing.
You may have remembered the concept of peaks and troughs, mountains and valleys. Cortisol spiking during the day and decreasing towards the evening. Melatonin increasing and spiking in the evening to night, and decreasing towards the day. Same for another hormones, endogenously. Growth hormone carries this same rhythm too, being released in a pulsatile manner during sleep, with its own built in inhibition during sleep. But with exogenous dosing, there also is a rhythm that is to be respected to get 'the most' out of it.
-----
GH Receptor Desensitization: The JAK2/STAT5 Axis
Continuing from the second point above, where GH binds to GH receptors and then the downstream signaling to make circulating IGF-1, there's also actions that occur causing rapid, multilayered desensitization from continued (ED) GH exposure.
-----
Negative Feedback: Somatostatin and IGF-1 Long-Loop Suppression
The picture becomes more complex at the hypothalamic-pituitary axis (HPA) level. Exogenous GH engages at least three layers of negative feedback:
GH itself acts at the hypothalamus to stimulate SRIF (somatostatin) secretion and suppress GHRH release. After a single sc GH injection in rats, endogenous pulsatile GH secretion was markedly suppressed for up to ~4 hours post-injection, with this feedback effect mediated at least in part by increased hypothalamic SRIF secretion. After this ~4-hour window, endogenous GH secretion began recovering, fully normalizing by 4–8 hours post-injection. Importantly, this time course did not change after 5 days of repeated GH administration in that study.

This is the more consequential feedback for dosing rationale. Circulating IGF-1 stimulates hypothalamic somatostatin release and suppresses both GHRH and pituitary GH secretion. During a 48-hour rhIGF-1 (recombinant human IGF-1) infusion in men, endogenous GH secretion was suppressed by 85%, primarily through attenuation of GH pulse amplitude (77% suppression), mediated by increased hypothalamic somatostatin secretion. GH response to exogenous GHRH was also suppressed by 82% during IGF-1 infusion.
Given that exogenous GH produces elevated IGFBP-3-bound IGF-1 with a half-life of 12–15 hours, ED dosing creates a near-continuous state of elevated circulating IGF-1 that persistently drives somatostatin tone and suppresses endogenous GH pulsatility. With 24-hour dosing intervals and an IGF-1 signal lasting 12–24 hours post-injection, there is essentially zero trough: no window for the hypothalamus to recover its GHRH drive or for somatostatin tone to fall back to baseline.
In contrast, EOD dosing provides a ~24-hour window (hours 24–48) in which:

-----
Clinical Evidence: Target-Organ Tolerance and Withdrawal
The most compelling clinical evidence comes from the Lampit & Hochberg (2002) study in children with idiopathic short stature (ISS) given equivalent weekly doses of GH (6 mg/m² weekly) as either daily or alternate-day injections:
Critically, post-treatment GH secretion, serum IGF-1, and IGF-1 binding proteins returned to normal in both groups, ruling out pituitary suppression as the mechanism. The authors concluded tolerance was at the target organ/GHR level in response to unphysiological pharmacokinetics of daily injection.
A separate study documented GH withdrawal syndrome persisting for up to 18 months after daily GH therapy in prepubertal children: also with normal post-treatment GH/IGF-1 levels, attributing it to dependence at the target organ level
An adult alternate-day rhGH study confirmed that EOD dosing produces comparable changes in IGF-1 levels, body fat percentage, and lipid profile to daily dosing: with potentially improved glucose tolerance handling

Table format for why ED GH dosing makes a pharmacodynamic dead zone and why EOD GH is better:
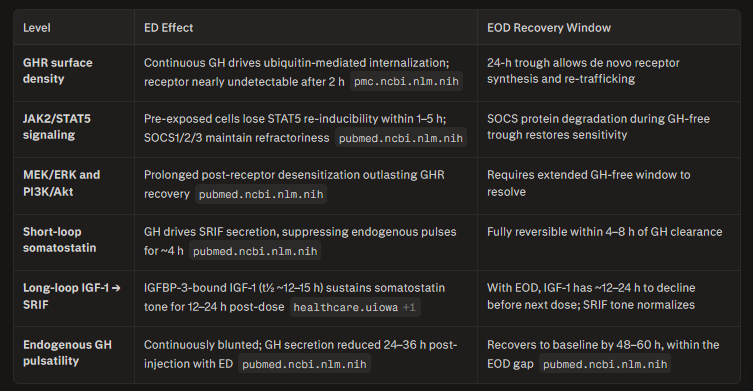
The net result is that ED dosing keeps the system in a state of tonic, non-pulsatile GH signaling: an unphysiological profile that the receptor machinery recognizes through the same desensitization mechanisms it would activate in response to a constitutively secreting somatotroph adenoma.
It is precisely the pulsatility of endogenous GH (high amplitude peaks followed by undetectable troughs) that maintains full GHR expression and JAK2/STAT5 signaling capacity; a pulsatile GH profile cycling receptors between activation and resensitization sustains downstream sensitivity far better than continuous or near-continuous occupancy.
EOD dosing preserves that pulsatile logic even for exogenous GH: each injection is a discrete, high-amplitude pulse followed by full pharmacological clearance and a receptor recovery window long enough (>24 h) to restore signaling competence across all three desensitization tiers before the next dose arrives.
-----
Layman's analogy: The Nightclub Bouncer
Imagine your cells have a bouncer at the door (the GH receptor). The bouncer's job is to let GH into the cell so it can do its work: to build muscle, burn fat, produce IGF-1.
Here's the problem: every time the bouncer lets GH in, he gets tired and needs to rest. If you keep sending GH to the door every single day, the bouncer is permanently exhausted, stops letting GH in effectively. You're paying for the VIP guest (GH) but he never gets past the door.
EOD dosing gives the bouncer a full rest day. By the time the next dose of GH arrives, the bouncer is fresh, alert, and lets everything through at full efficiency.
The Three Simple Reasons:
1. The receptor gets worn out with daily use.
When GH hits its receptor, the cell actually pulls the receptor inside and destroys it as part of the normal signaling process. The cell needs roughly 24+ hours to build new receptors and put them back on the surface. With daily (ED) dosing, you're knocking on a door that has already been taken off its hinges — GH shows up but there's nothing to bind to.
2. Your body fights back harder with daily dosing.
When GH is detected in the bloodstream, the brain responds by releasing somatostatin: a hormone whose only job is to suppress GH activity. It's the body saying "we have enough, stop." Exogenous GH also triggers your liver to produce IGF-1, which sends the same suppression signal back to the brain. IGF-1 hangs around in the blood for 12–15 hours after a GH injection. With daily dosing, you never leave this suppression window: your own biology is continuously working against the GH you're injecting. With EOD dosing, IGF-1 has time to fall back toward baseline, somatostatin tone drops, and the axis "forgets" it was suppressed before the next dose.
3. Your own natural GH secretion gets shut down permanently with daily dosing.
Healthy people release GH in pulses: big spikes followed by complete troughs, especially during deep sleep. These natural pulses require the troughs to work, because the pituitary gland needs the low period to refill its GH stores and become responsive again. Daily exogenous GH eliminates these troughs entirely. EOD dosing preserves at least one full day where your pituitary can fire naturally, keeping the system "warm" rather than fully suppressed.
The One-Sentence Version:
"With daily GH injections, your body's receptors wear out, your brain actively fights the GH with suppression signals, and your own natural GH production shuts off: you end up paying for a compound that's increasingly ignored. Skipping a day lets all three of those systems reset, so each injection actually works."
I know I got 2 peeps @DispoH3R0 and @JewBastard18 doing this, no idea who else
Don't react, just try it. Some day is in the screenshots below


Now to answer the contexted question:
"Why would a secretagogue be used between days of EOD GH use? I thought GH receptors were desensitized?"
"How can ED dosing of GH contribute to increased side effects frequently spoken about? With GH receptor desensitization/downregulation, doesn't that mean there shouldn't be side effects with ED dosing? (Examples of ED GH dosing side effects: acromegaly, swelling, carpal tunnel; some have anecdotally reported reduction of these side effects when switching to EOD GH dosing)"