Statins work by inhibiting the HMG-CoA reductase enzyme. Variations in the HMGCR gene work by affecting HMG-CoA reductase enzymatic activity.
The metabolic effect of variation in HMGCR and of taking statins is virtually identical.
This gives us a great natural experiment🧵


If you're wondering about the effects of taking statins over long periods of time, look no further than people with genetically low cholesterol due to variants in HMGCR.
Compared to starting statins later in life, those with genetically low LDL have 3x lower heart disease risk!
Compared to starting statins later in life, those with genetically low LDL have 3x lower heart disease risk!

Not only that, but the safety profile of low LDL is phenomenal.
People with low LDL do as well or better on most health dimensions.
So, TL;DR: It's great and statins are safe. Thank you, genetic freaks.
People with low LDL do as well or better on most health dimensions.
So, TL;DR: It's great and statins are safe. Thank you, genetic freaks.
Some people can't take statins because they experience myopathy due to genetic variation in HMGCR.
So, they take drugs like PCSK9 inhibitors or ezetimibe instead.
Genetic variation mimicking ezetimibe? Metabolically almost identical to genetic variation mimicking statins:
So, they take drugs like PCSK9 inhibitors or ezetimibe instead.
Genetic variation mimicking ezetimibe? Metabolically almost identical to genetic variation mimicking statins:

Accordingly, when it comes to ezetimibe, we can pretty much port over the safety profile of statins, plus or minus whatever is directly on the drug's mechanistic pathway.
We do port, say, reduced heart disease risk, but we don't port the mevalonate-based myopathy risk.
We do port, say, reduced heart disease risk, but we don't port the mevalonate-based myopathy risk.
As an example of this, the result (shown below) for ezetimibe shows the effects of having higher predicted effects like ezetimibe genetically on one's risk of cancer.
There's no risk. There's also no risk from statins. We could've probably figured that out with the one study.
There's no risk. There's also no risk from statins. We could've probably figured that out with the one study.

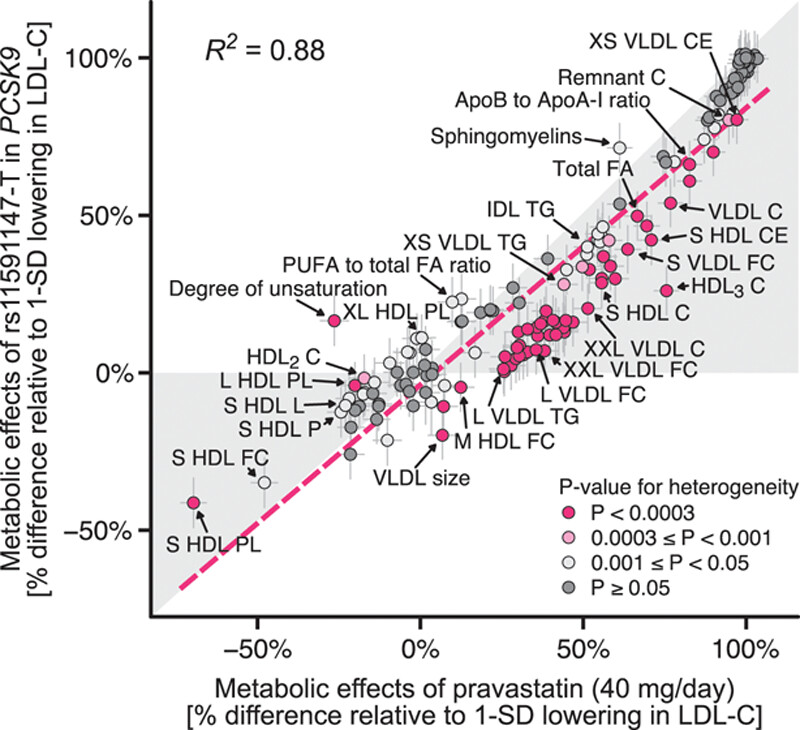
We can also mostly do the same thing with PCSK9 inhibitors, but we're somewhat more limited.
We're more limited because PCSK9 inhibitors aren't quite as effective at lowering very-low-density lipoprotein, so they work somewhat differently.
But they're still broadly similar!
We're more limited because PCSK9 inhibitors aren't quite as effective at lowering very-low-density lipoprotein, so they work somewhat differently.
But they're still broadly similar!
All of this is to say:
1. You can learn about long-term use effects from genetic variation, and
2. You can learn about drugs from other, highly similar drugs.
This is like a cheat code to understanding drug risk, and it's something you can easily go and check right now.
1. You can learn about long-term use effects from genetic variation, and
2. You can learn about drugs from other, highly similar drugs.
This is like a cheat code to understanding drug risk, and it's something you can easily go and check right now.
As I argued in my latest article, this is something Regeneron will now be doing since they've just acquired the data to do it with an unprecedented level of clarity and scale.
Go check that out: cremieux.xyz/p/the-23andme-…
Go check that out: cremieux.xyz/p/the-23andme-…
P.S. The broad "no risk" judgment for cancers refers to a clumped category including all cancers.
That leaves the possibility that these drugs raise the risk of some and lower the risk of others. They don't seem to, but maybe I'm missing the right cancers.
That leaves the possibility that these drugs raise the risk of some and lower the risk of others. They don't seem to, but maybe I'm missing the right cancers.
P.P.S. Why yes, I have been using this same genetic natural experiment strategy to vet claims like 'GLP-1RAs make people relatively fatter' and 'GLP-1RAs cause thyroid cancer.'
No on both counts.
Find some of that here: cremieux.xyz/p/ozempic-and-…
No on both counts.
Find some of that here: cremieux.xyz/p/ozempic-and-…

Locked follower shares another natural experiment:
Families with hypercholesterolemia.
Statins weren't available in the parent generation, but for their kids, they got statin therapy. As a result, they got to age 39 with far fewer cardiovascular problems and lower mortality.
Families with hypercholesterolemia.
Statins weren't available in the parent generation, but for their kids, they got statin therapy. As a result, they got to age 39 with far fewer cardiovascular problems and lower mortality.

Because of the wonders of statins, these kids were able to live normal lives and progress to midlife without incident.
Compared to their parents? Way better. Compared to their siblings without the condition? No different.
Statins save lives.
Compared to their parents? Way better. Compared to their siblings without the condition? No different.
Statins save lives.
Source: nejm.org/doi/full/10.10…
Generated by Thread Navigator
Press ⌘ + S to quick-export