@hjluks: Pain on the outside of your sh...
@hjluks
10 views
Mar 26, 2026
Advertisement
1
Pain on the outside of your shoulder is also one of the most common problems I see in my practice.
Lifters get it. Swimmers get it. Pickleball players get it. People who haven't lifted their arm overhead in years get it.
For decades, we called it impingement and blamed a bone spur. That led to many unnecessary bone removal surgeries. We were treating the wrong thing.
Lifters get it. Swimmers get it. Pickleball players get it. People who haven't lifted their arm overhead in years get it.
For decades, we called it impingement and blamed a bone spur. That led to many unnecessary bone removal surgeries. We were treating the wrong thing.
2
The problem is usually due to the rotator cuff tendons, not the bursa. Sometimes it's both.
Think of it like the gluteal tendons at the hip. The bursa gets irritated, but it is reacting to what is happening next door.
Both the shoulder and hip can hurt without a significant tear. Many patients with the worst shoulder pain have an intact rotator cuff. Shoulder pain does NOT correlate with the size of a tear.
Sleeping at night!! Why does it hurt so much at night?!?!
Both the gluteal tendons and cuff can show tears on imaging without causing pain.
Both sets of tendons strain when the load exceeds their capacity.
Both respond best to progressive strengthening.
Think of it like the gluteal tendons at the hip. The bursa gets irritated, but it is reacting to what is happening next door.
Both the shoulder and hip can hurt without a significant tear. Many patients with the worst shoulder pain have an intact rotator cuff. Shoulder pain does NOT correlate with the size of a tear.
Sleeping at night!! Why does it hurt so much at night?!?!
Both the gluteal tendons and cuff can show tears on imaging without causing pain.
Both sets of tendons strain when the load exceeds their capacity.
Both respond best to progressive strengthening.
3
This is very often a capacity problem, not an inflammation problem. The inflammation is often secondary. But calcium in the cuff and a frozen shoulder are definitely inflammatory... just not as common as cuff-related pain.
The cuff tendons are being asked to do more than they are currently prepared for. That gap opens slowly, from deconditioning, a change in activity, years of avoiding strength work, or the metabolic shifts that come with age, menopause, insulin resistance, or thyroid disease.
Poor metabolic health is not well tolerated by the cuff tendons. Menopause related shoulder pain can be awful, too.
The tendon does not fail dramatically. It just stops tolerating what it used to tolerate without complaint.
Most people with shoulder pain have no history of falls or injury.
The cuff tendons are being asked to do more than they are currently prepared for. That gap opens slowly, from deconditioning, a change in activity, years of avoiding strength work, or the metabolic shifts that come with age, menopause, insulin resistance, or thyroid disease.
Poor metabolic health is not well tolerated by the cuff tendons. Menopause related shoulder pain can be awful, too.
The tendon does not fail dramatically. It just stops tolerating what it used to tolerate without complaint.
Most people with shoulder pain have no history of falls or injury.
4
Two things people do that backfire:
Rest. The tendon's capacity keeps falling. When you resume normal activity, the pain returns, and now you are weaker than when you started.
Stretching. Aggressive stretching in the early, irritated phase compresses the tendon and prolongs the irritation.
The tendon does not need protection. It needs a progressive load.
Rest. The tendon's capacity keeps falling. When you resume normal activity, the pain returns, and now you are weaker than when you started.
Stretching. Aggressive stretching in the early, irritated phase compresses the tendon and prolongs the irritation.
The tendon does not need protection. It needs a progressive load.
5
Tendons heal under load. Appropriate, progressive load.
Early on: isometric external rotation holds, I-Y-T exercises with light dumbbells, and supported cuff activation.
Later: resisted external rotation, rows, farmer carries, and eventually controlled overhead work.
Most lateral shoulder pain is not a structural disaster. It is a tendon that was not prepared for the demands placed on it. Again... the tendons are also exquisitely sensitive to metabolic health and to estrogen loss.
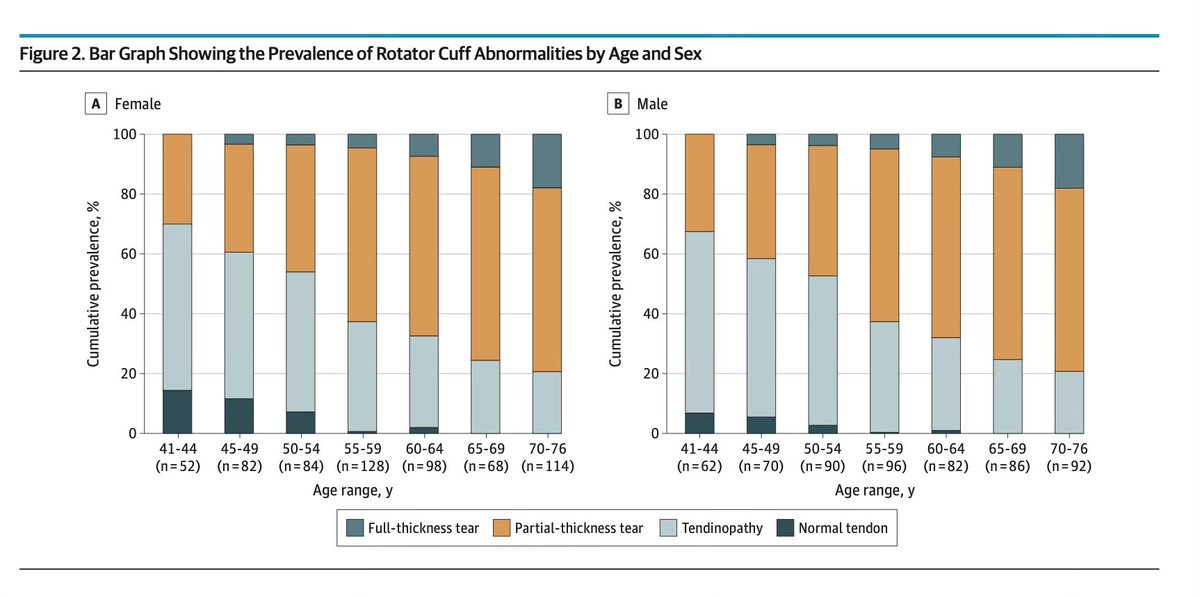
Even if a small "tear" exists. The research is clear... the majority do not need surgery. Many are age-appropriate changes.
Nearly 95% of people over 40 have changes in the rotator cuff on MRI! Your MRI will not say "normal."
Build that preparation, and most people return to everything they care about. But it can take many months.
Early on: isometric external rotation holds, I-Y-T exercises with light dumbbells, and supported cuff activation.
Later: resisted external rotation, rows, farmer carries, and eventually controlled overhead work.
Most lateral shoulder pain is not a structural disaster. It is a tendon that was not prepared for the demands placed on it. Again... the tendons are also exquisitely sensitive to metabolic health and to estrogen loss.
Even if a small "tear" exists. The research is clear... the majority do not need surgery. Many are age-appropriate changes.
Nearly 95% of people over 40 have changes in the rotator cuff on MRI! Your MRI will not say "normal."
Build that preparation, and most people return to everything they care about. But it can take many months.
6
Injections into the bursa can facilitate rehab. Calcium, if present, can be washed out with a needle and rarely requires an operation.
Cortisone injections into the bursa can work well in some cases... PRP might work well for tendinopathy that doesn't respond to rehabilitation alone.
But rehab, mobility, and strength training are the primary goals of a good treatment program.
howardluksmd.substack.com/p/why-does-the…
Cortisone injections into the bursa can work well in some cases... PRP might work well for tendinopathy that doesn't respond to rehabilitation alone.
But rehab, mobility, and strength training are the primary goals of a good treatment program.
howardluksmd.substack.com/p/why-does-the…
7
Pain on the outside of your hip is one of the most common problems I see in my practice.
Walkers get it. Runners get it. People who've never been to a gym get it.
For decades, we called it bursitis and injected it. We were treating the wrong thing.
Walkers get it. Runners get it. People who've never been to a gym get it.
For decades, we called it bursitis and injected it. We were treating the wrong thing.